
PCOS and Hypothyroidism #22
What is the link between PCOS and Hypothyroidism?

Hello lovely people,
I am writing to you today from beautiful Romania. We are on a road trip with our families, visiting the beautiful Carpathian Mountains.

Today’s topic touches on another chronic condition emerging in PCOS discussions. A dear reader asked this question a few months ago:
What is the link between PCOS and Hypothyroidism?
Hypothyroidism or an underactive thyroid gland is a condition where the thyroid gland does not produce enough thyroid hormones.
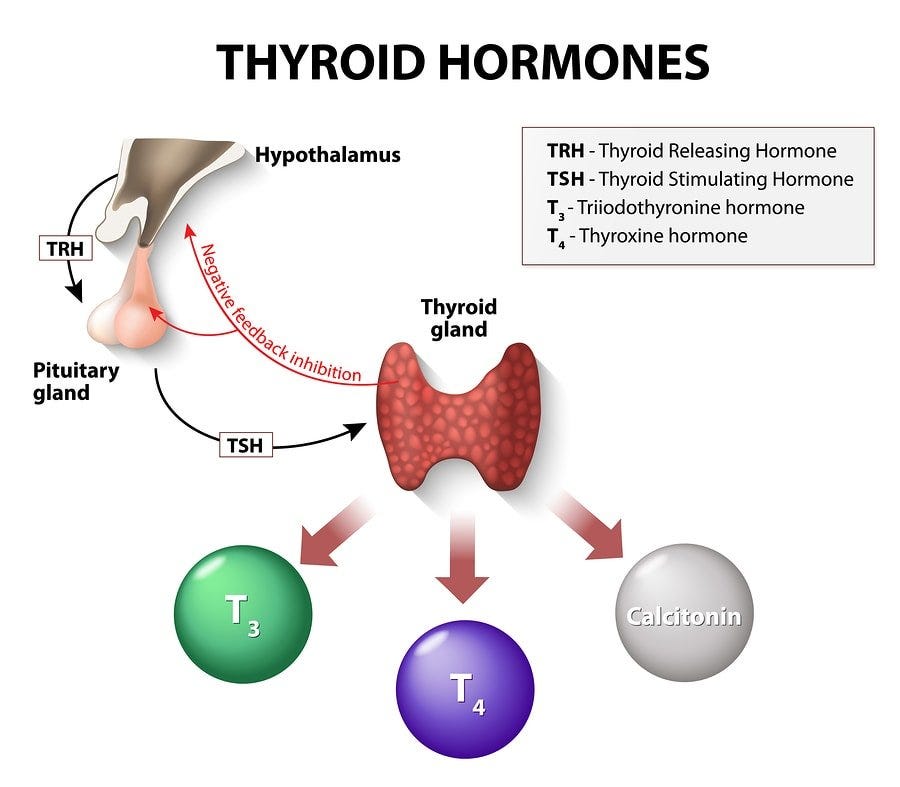
The thyroid produces and releases into the circulation at least two potent hormones, thyroxine (T4) and triiodothyronine (T3). The hormones influence metabolic processes, brain function, including intelligence and memory, neural development and bone development. T3 and T4 are produced under the influence and THR (Thyrotropin-releasing hormone) and TSH (Thyroid Stimulating Hormone). These hormones get released from the same organs as our LH and FSH: Hypothalamus and Pituitary Gland.
The main job of the thyroid is to control our metabolism. Metabolism is the process that our body uses to transform food into energy. The thyroid creates the hormones T4 and T3 to control our metabolism. These hormones work throughout the body to tell the body’s cells how much energy to use. They also control our body temperature and heart rate.
In the case of an Underactive thyroid, the thyroid cannot stimulate the production of enough T3 and T4 and is compensated with high levels of TSH. The brain is trying to stimulate the thyroid to produce these hormones and as a result, it increases TSH.
Its primary symptoms are fatigue, lethargy, cold intolerance, brain fog, slowed reflexes, hair loss, dry skin, weight gain, and constipation.
The most common cause of hypothyroidism is chronic autoimmune thyroiditis (Hashimoto's disease), in which the thyroid is attacked by our immune system. Other causes are radioactive iodine, thyroid inflammatory disease, iodine deficiency, and several drugs that interfere with thyroid hormones.
How does it link to PCOS?
Interestingly, a study on 827 women found Hashimoto’s thyroiditis to be three times more common in women with PCOS (what a joy, another increased risk factor for us).
Another finding within this study was that those women who had both Hashimoto and PCOS had less androgens, but posed a higher metabolic risk and were more obese.
There are two theories by which these two conditions seem to be discussed together:
1. Prolactin effect on the ovaries
As TRH (Thyrotropin-releasing hormone) stimulates the Pituitary Gland to create TSH (Thyroid Stimulating Hormone), it also stimulates the production of Prolactin.
Prolactin = a hormone which is high during pregnancy and stimulates milk production and the development of mammary glands within breast tissues
High levels of prolactin stop ovulation. This is why breastfeeding women (and thus have high prolactin levels) usually don't become pregnant as they don’t ovulate. Prolactin stops ovulation by inhibiting FSH (Follicle Stimulating Hormone) secretion.
Given ovulation doesn’t happen, follicles within the ovaries don’t mature and as a result, cysts become present in the ovaries. Women with hypothyroidism often have polycystic ovaries due to the mechanism described above. Due to this, irregular periods can also be seen in women with hypothyroidism. This is one of the reasons why these two conditions are discussed together. In fact, thyroid disorders are one of the exclusion criteria before diagnosing PCOS.
While women with hypothyroidism might have polycystic ovaries, it doesn’t mean they will have the syndrome. There is no evidence to suggest that primary hypothyroidism can lead to PCOS, and these two conditions might develop independently.
2. Obesity’s influence on hypothyroidism and PCOS
Both hypothyroidism and PCOS are often linked to insulin resistance and weight gain.
In hypothyroidism, proinflammatory molecules and insulin resistance seem to directly impact the Pituitary gland and increase the level of TSH. Increased leptin in obesity has also been proposed to act on the hypothalamus resulting in increased TSH secretion.
Given insulin resistance and excess fatty tissue is also present in PCOS, these conditions might be linked. However, PCOS has not been proven to be caused by insulin resistance, and hypothyroidism is primarily an auto-immune condition. So these conditions seem to share a similar mechanism, there isn’t a clear link between the two.
Checking your thyroid
If you have PCOS, you should also check your thyroid regularly. TSH and T4 are relatively inexpensive blood tests and are often part of routine tests done by doctors.
Keeping the thyroid healthy
There are some essential nutrients we must get in reasonable quantities to maintain a healthy thyroid:
Tyrosine and iodine: the raw materials T3 and T4 are made out of
Iron: helps with the conversion of T4 to T3
Selenium and zinc: Enzyme co-factors
Vitamin D: Immune modulation
Vitamins A, C, E, B2, B3, B6, B12: Support synthesis and function.
Copper: A cofactor in enzymes
I hope you enjoyed reading about the link between these two conditions. I am hoping in the following newsletters to start unpacking other common conditions that PCOS is associated with.
Wishing you a lovely Sunday,
Francesca
1 Sources
Institute of Medicine (US) Committee on Medicare Coverage of Routine Thyroid Screening, Stone, M. B., & Wallace, R. B. (2003). Pathophysiology and diagnosis of thyroid disease. National Academies Press.
Saran, S., Gupta, B. S., Philip, R., Singh, K. S., Bende, S. A., Agroiya, P., & Agrawal, P. (2016). Effect of hypothyroidism on female reproductive hormones. Indian Journal of Endocrinology and Metabolism, 20(1), 108–113. https://doi.org/10.4103/2230-8210.172245
Singla, R., Gupta, Y., Khemani, M., & Aggarwal, S. (2015). Thyroid disorders and polycystic ovary syndrome: An emerging relationship. Indian Journal of Endocrinology and Metabolism, 19(1), 25–29. https://doi.org/10.4103/2230-8210.146860
Ulrich, J., Goerges, J., Keck, C., Müller-Wieland, D., Diederich, S., & Janssen, O. (2018). Impact of autoimmune thyroiditis on reproductive and metabolic parameters in patients with polycystic ovary syndrome. Experimental and Clinical Endocrinology & Diabetes, 126(04), 198–204. https://doi.org/10.1055/s-0043-110480