
PCOS and Cholesterol #24
Is high Cholesterol linked to PCOS?

Hello all,
I hope you are enjoying the summer sun. London has been pretty hot over the past week. In today’s newsletter, we will discuss Cholesterol and how it links to PCOS.
This week’s question
Is high Cholesterol linked to PCOS?
What is Cholesterol?
Cholesterol is a type of fat which is made in the liver. Cholesterol is also present in foods, although only 20% comes from alimentation. Our liver makes 80% of it. But why does our body produce so much cholesterol?
Cholesterol is pretty much vital for our body:
Cholesterol forms part of each cell wall, helping keep its integrity.
Our dear, Oestrogen and Testosterone starts as Cholesterol and gets synthesised into the hormones we need.
Cholesterol is needed to digest fats as it’s a key component of bile.
We need Cholesterol in our skin cells to make vitamin D from sunlight.
Why does it get such a bad rep?
Cholesterol is a type of fat. As you might remember from our chemistry classes, fat and water don’t mix. As a result, for cholesterol to travel from the liver to where it’s needed, it uses specific lipoproteins to hop on and hop off when needed (🚌 like the red tourist’s buses). The two most commonly known lipoproteins are low-density lipoproteins (LDL) and high-density lipoproteins (HDL).
Low-density lipoproteins (LDL) carry cholesterol from the liver to the rest of the body. Cells latch onto these particles and extract fat and cholesterol from them. When there is too much LDL cholesterol in the blood, these particles can form deposits in the walls of arteries throughout the body. This is why it’s often referred to as bad cholesterol.
High-density lipoproteins (HDL) hunt cholesterol from the bloodstream, LDL, and artery walls and takes it back to the liver for disposal. Think of HDL as the garbage trucks of the bloodstream. HDL cholesterol is often called good cholesterol because it helps keep LDL within a healthy range.
High levels of LDL can cause plaque buildup. However, it is not only the amount that is problematic; it’s their oxidation. By oxidising, the immune system is alerted through inflammatory markers such as IL6 (Interleukin 6). Immune cells are recruited to absorb this oxidised cholesterol, but with added oxidation, it can create a plaque over time. The existence of these plaques gets referred to as atherosclerosis. Over time, this plaque can obstruct the blood flow in an artery, leading to a blockage. Depending on where it happens, this blockage can lead to a stroke or heart attack.
Oxidation cannot be avoided because even when our cells produce energy (ATP), it creates oxidation. This is within a manageable quantity. However, diets high in sugars, trans fats, exposure to pollution, smoking, toxin and consumption of alcohol all raise oxidation, raising our risk of plaque formation and heart disease.
How does it link to PCOS?
I feel like I always bring bad news…
According to the National Cholesterol Education Program (NCEP), approximately 70% of PCOS women have abnormal cholesterol levels. We seem to exhibit lower levels of HDL and higher levels of LDL. Great news.
It is fascinating to me how everything is so interlinked. Every time I read about one specific topic, it always comes back to excess fat tissue (the one around our waist), raised androgens and increased insulin resistance. What is responsible for our PCOS symptoms often impacts other health markers. This is how it impacts cholesterol:
Testosterone has been implicated in lowering HDL levels. The effects of testosterone have been mainly attributed to the up-regulation of two genes involved in HDL: receptor B1 (SR-B1) and hepatic lipase (HL).
Excess fat tissue and insulin resistance have been positively correlated with LDL levels by driving the overproduction of smaller and denser LDL proteins, resulting in more fat-rich particles and less HDL.
What can we do about it?
Here are my top recommendations if you are worried about your cholesterol levels:
Fibre, particularly soluble fibre, has been associated with decreased LDL levels. Soluble fibre becomes a thick gel in our intestines, slows digestion (which keeps blood sugars from spiking) and traps fats so they can't all be absorbed (lowering cholesterol levels). In addition, cholesterol is secreted via our poo. Maintaining regular bowel movements ensures we remove excess cholesterol from our bodies. I have a comprehensive guide on the importance of fibre here, including examples of foods and how to get enough of it in your diet.
Antioxidants: consuming a diet rich in antioxidants ensures that we offer our body the ability to fight oxidation. The more colourful the foods are, the higher in antioxidants.
Plant stanols and sterols: they have a similar chemical structure to cholesterol. They are thought to work by reducing cholesterol absorption in the gut so more is lost in the poo. Evidence shows that eating 2g (between 1.5g to 3g) of plant stanols and sterols can lower LDL. Food high in stanols and sterols are cereals, rice bran and nuts. It’s pretty hard to get 2g of these nutrients without consuming a high carbohydrate diet, so a supplement might be something to consider.
Reducing the consumption of trans-fats: healthy sources of fats (olive oil, avocado, nuts, fish) should be a key component of our diet. However, processed foods high in trans fats (fried foods, cakes, margarine) should be consumed in small quantities.
Regular exercise: cardiovascular and resistance training has been shown to reduce LDL and boost HDL cholesterol.
There are also medications to help lower Cholesterol. Discussing your plan to lower cholesterol with your GP should be a priority if you are worried about your blood markers.
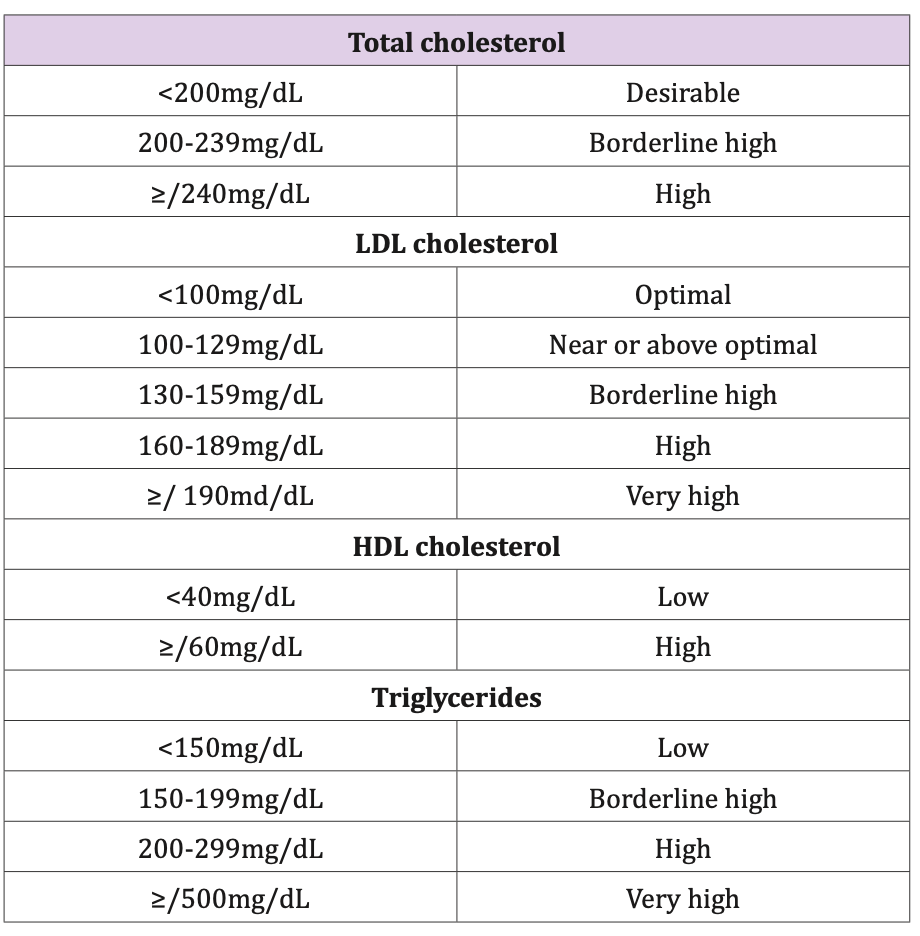
Testing for Cholesterol
Cholesterol tests are very cheap to get and form part of routine testing. I keep a close eye on mine every 3-6 months. These are the references:
I hope you have enjoyed this newsletter. If you have questions you’d like me to answer, please don’t hesitate to submit them here or comment on this post.
See you next Sunday,
Francesca
1 Reference
Bereda G. (2022) Pathophysiology and Management of Dyslipidaemia. Biomed J Sci & Tech Res 43.
Cholesterol. (2014, June 9). The Nutrition Source. https://www.hsph.harvard.edu/nutritionsource/what-should-you-eat/fats-and-cholesterol/cholesterol/
Diamanti-Kandarakis, E., Papavassiliou, A. G., Kandarakis, S. A., & Chrousos, G. P. (2007). Pathophysiology and types of dyslipidemia in PCOS. Trends in Endocrinology and Metabolism: TEM, 18(7), 280–285. https://doi.org/10.1016/j.tem.2007.07.004
Howard, B. V. (1999). Insulin resistance and lipid metabolism. The American Journal of Cardiology, 84(1A), 28J-32J. https://doi.org/10.1016/s0002-9149(99)00355-0
Mann, S., Beedie, C., & Jimenez, A. (2014). Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and the lipid profile: review, synthesis and recommendations. Sports Medicine (Auckland, N.Z.), 44(2), 211–221. https://doi.org/10.1007/s40279-013-0110-5
Disclaimer: We are all unique in our ways, so this information is for educational purposes only. In my communications, I summarise research data and bring my experience. This shouldn’t be viewed as medical advice at any point. Please further consult your healthcare provider about your health needs.