
There's a surgery that can restart ovulation in PMOS
Why has no one told you about it?

Hello everyone,
Is there a surgery that could fix my PMOS?
Trying to ovulate with our condition is challenging. There are multiple medication options to try, but if they fail, the current guidelines recommend ovarian drilling. Did you know this was an option?
I have been meaning to write about ovarian drilling for a long time, as a company is currently developing and conducting a clinical trial in the US for an innovative version of this surgery.
Ovarian drilling was, in 1984, one of the only treatments available for what we now call PMOS, and then it quietly disappeared from the conversation, but it’s still available today. I must admit, they should find a nicer name for it because having my ovaries drilled sounds scary.
What is ovarian drilling?
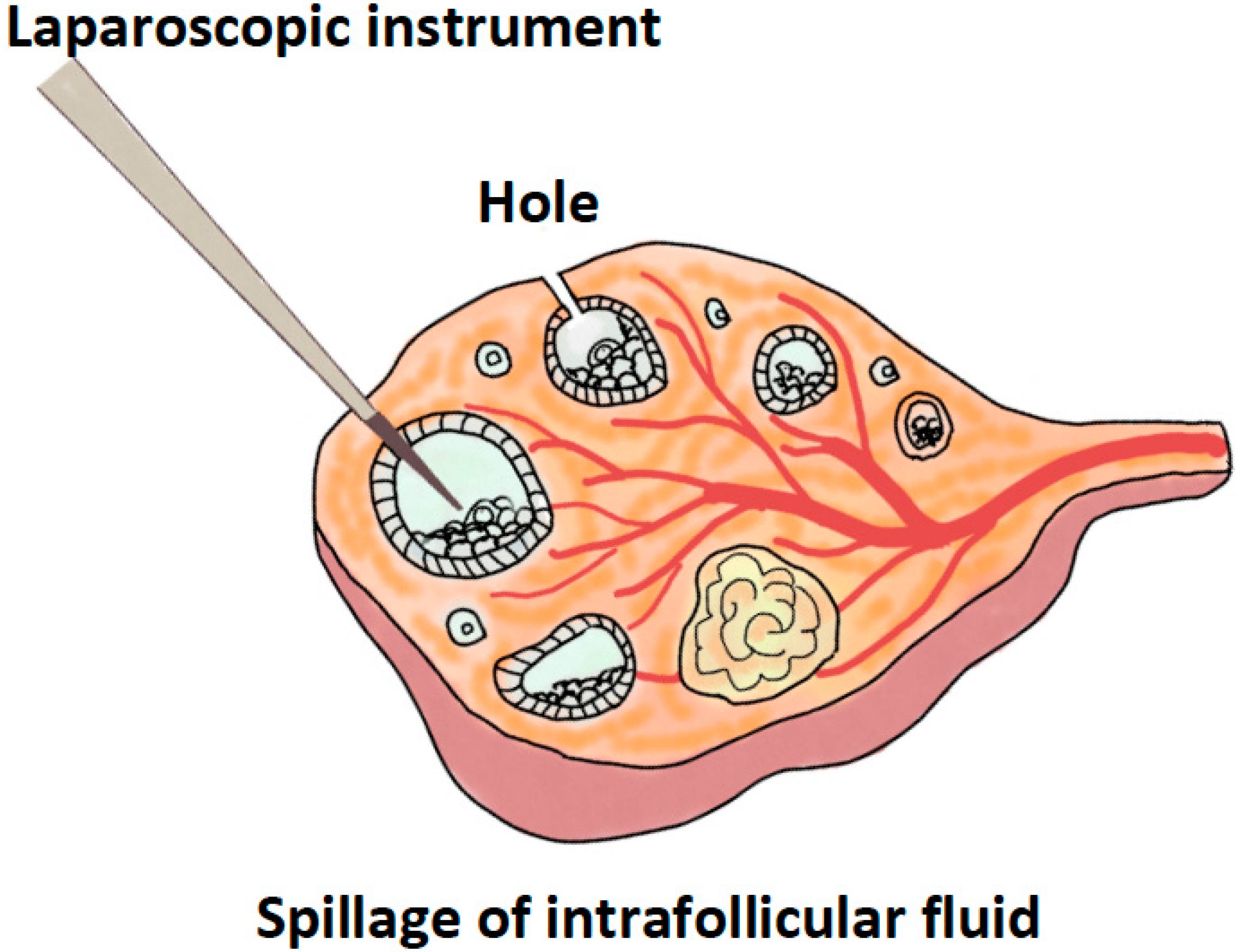
Laparoscopic ovarian drilling (LOD) is a minor surgical procedure performed under general anaesthetic. A surgeon makes a small incision in the abdomen, inserts a thin camera (a laparoscope), and uses either heat or laser energy to create small punctures across the surface of each ovary.
It sounds more dramatic than it is. It is done as day surgery and most women go home the same day.
This technique is not new. It evolved from a much older procedure called ovarian wedge resection, first described by Stein and Leventhal in 1935, which involved surgically removing a wedge of ovarian tissue via open abdominal surgery. It was effective at restoring ovulation, but carried a significant risk of scarring inside the pelvis and was largely abandoned once clomiphene citrate (a fertility tablet) became available in the 1960s. Laparoscopic ovarian drilling was first described in 1984 as a minimally invasive alternative: the same physiological rationale, achieved with a far less traumatic approach.
What I find interesting is that for decades it fell largely out of favour — not because it stopped working, but because fertility drugs became easier to prescribe. It is only now, as researchers take a harder look at the long-term data, that it is being reconsidered more seriously.
How does it work?
To understand the mechanism, it helps to revisit what is actually happening in the PMOS ovary.
As we have covered in previous issues, a defining feature of PMOS is excess androgen production within the ovary itself. This disrupts the relationship between LH (luteinising hormone) and FSH (follicle-stimulating hormone), the two signals the brain sends to the ovaries to coordinate ovulation.
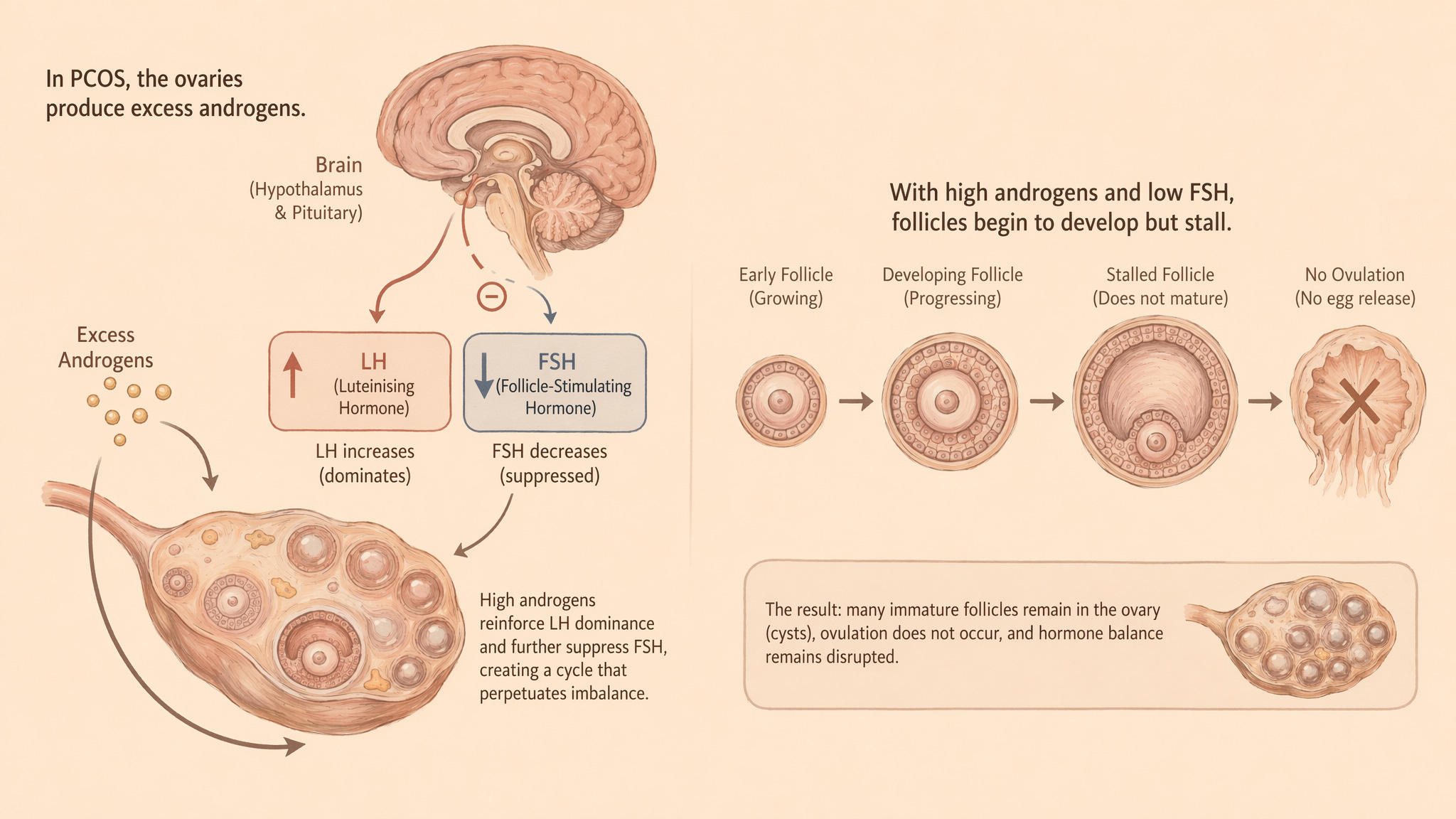
When androgens are too high, LH dominates, FSH is suppressed, and follicles stall. They begin to develop but never fully mature or release an egg.
I want to be honest here about what is and is not known, because the mechanism of LOD is more uncertain than it is often presented.
The most supported hypothesis works as follows:
→ the thermal energy from the drilling needle destroys a portion of the androgen-producing tissue inside the ovary.
→ this produces a local inflammatory response and leads to drainage of what researchers describe as “toxic” follicular fluid — the fluid surrounding those stalled, immature follicles.
→ the downstream effects are a reduction in androgen levels, a fall in LH, and a normalisation of the hypothalamic-pituitary-ovarian (HPO) axis, the communication loop between the brain and the ovaries.
→ with less androgens, FSH signalling can resume and normal follicular recruitment restarts.
This is what they think is happening, but it is not clear.
What does it do for PMOS/PCOS?
Studies report spontaneous ovulation rates ranging from 30% to 90% and cumulative pregnancy rates from 13% to 88%. These ranges are huge, which makes me question the quality of evidence.
The most rigorous assessment of LOD we have is a 2020 systematic review that pooled 38 randomised controlled trials involving over 3,300 women. Here is what it actually found:
With low-quality evidence, LOD may slightly lower live birth rates compared to medical ovulation. To put numbers to that: if medication alone gives a 42% live birth rate, LOD gives you somewhere in the region of 28–40%. That sounds like a meaningful gap. But here is the thing — when the researchers zoomed in on only the trials with the most rigorous methodology, that difference disappeared completely. The honest conclusion from the best available evidence is that we genuinely do not know whether LOD is better, worse, or the same as medication when it comes to live birth rates.
It can reduce the risk of multiple pregnancy, twins or more. Injectable fertility medications stimulate multiple follicles at once, which is where that risk comes from. LOD tends to induce one egg at a time, and the evidence is for a meaningfully lower multiple pregnancy rate.
LOD may also reduce the risk of ovarian hyperstimulation syndrome (OHSS), a potentially serious side effect of hormonal stimulation.
Overall, the authors rated the evidence as very low to moderate quality. The main issues are inconsistent surgical techniques across studies and poor reporting of how patients were assigned to groups.
This is where it gets particularly relevant for those of us in the UK.
LOD is not fringe or experimental. It is listed in NICE’s fertility guidelines as one of three recommended second-line treatments for people with PMOS who have not responded to first-line medication, specifically those who are resistant to clomifene citrate (a common ovulation-inducing drug). The three options NICE recommends at this stage are:
Laparoscopic ovarian drilling
Combined clomifene citrate and metformin (if not already tried)
Gonadotrophins (hormone injections)
The choice between these depends on clinical circumstances and individual preference. So if you have tried first-line treatment without success, LOD is a legitimate conversation to have with a reproductive specialist and one the NHS is mandated to offer.
The practical reality, as with many NHS services, is that availability and waiting times vary significantly by trust. But knowing it exists on the pathway is the first step to being able to ask for it.
A small detail to bear in mind
There is something to consider:
AMH (anti-Müllerian hormone) is a marker for ovarian reserve, a measure of how many follicles remain. In women with PMOS, AMH is typically elevated, often two to three times higher than average, which reflects the large pool of small, stalled follicles.
After ovarian drilling, AMH levels drop. In most cases, this appears to represent a normalisation, coming down from an abnormally elevated level toward a healthier range. However, some studies have found more significant reductions, raising questions about whether aggressive or repeated drilling could affect long-term egg supply. A 2017 meta-analysis on this topic confirmed that LOD reduces AMH and antral follicle count, though the clinical significance is stil a bit in the air
What May Health is building on top of this
A California-based company called May Health is developing what they call the Anavi procedure, a modern iteration of ovarian drilling that does not require traditional laparoscopic surgery. Their approach uses targeted ovarian ablation in an outpatient setting, without the need for a general anaesthetic and the surgical infrastructure that currently comes with LOD.
The device has already received CE Mark certification in Europe, meaning it has cleared the regulatory bar for safety and performance here. They are currently running a clinical trial in the United States, the REBALANCE Study, seeking FDA approval.
The underlying biology is identical to that of traditional ovarian drilling: reduce androgen production at the ovarian level, restore hormonal feedback, and allow ovulation to resume. What May Health is attempting is to make that mechanism accessible without the barriers of general anaesthetic, operating theatre time, and surgical recovery. Whether the Anavi procedure achieves equivalent outcomes to traditional LOD is what their trial is designed to establish, and we do not have that data yet.
But the direction of travel is interesting. If the results hold, this could eventually become a far more accessible intervention relevant even for women who would not currently qualify for, or want, traditional surgery.
So, is this relevant to you?
Ovarian drilling is most likely to be considered if:
You have been diagnosed with PMOS and are not ovulating
You have not responded to first-line medications such as letrozole or clomiphene citrate
You are pursuing pregnancy and want to explore options before or instead of IVF
You are particularly motivated to find a hormone-free approach
It is not a lifestyle intervention and it is not a cure for PMOS in the broader sense, it does not address insulin resistance, inflammation, or the underlying genetic and metabolic drivers we have discussed before. But for the specific problem of anovulation, the evidence is accumulating and the field is moving.
What I keep coming back to is how quietly this procedure has been sitting in the evidence base since 1984, available on the NHS and yet how rarely it seems to come up in the conversations women with PMOS have with their doctors. It’s worth keeping an eye out for it.
See you next Sunday,
Francesca
Disclaimer: We are all unique in our own ways, so this information is for educational purposes only. In my communications, I summarise research data and bring my experience. This shouldn’t be viewed as medical advice at any point. Please further consult your healthcare provider about your health needs.
Sources
Bordewijk, E.M., Ng, K.Y.B., Rakic, L., Mol, B.W.J., Brown, J., Crawford, T.J. and van Wely, M. (2020) ‘Laparoscopic ovarian drilling for ovulation induction in women with anovulatory polycystic ovary syndrome’, Cochrane Database of Systematic Reviews, (2), p. CD001122. Available at: https://doi.org/10.1002/14651858.CD001122.pub5
Franik, S., Le, Q.K., Kremer, J.A., Kiesel, L. and Farquhar, C. (2022) ‘Aromatase inhibitors (letrozole) for ovulation induction in infertile women with polycystic ovary syndrome’, Cochrane Database of Systematic Reviews, (9), p. CD010287. Available at: https://doi.org/10.1002/14651858.CD010287.pub4
Yu, Q., Hu, S., Wang, Y., Cheng, G., Xia, W. and Zhu, C. (2019) ‘Letrozole versus laparoscopic ovarian drilling in clomiphene citrate-resistant women with polycystic ovary syndrome: a systematic review and meta-analysis of randomized controlled trials’, Reproductive Biology and Endocrinology, 17(1), p. 17. Available at: https://doi.org/10.1186/s12958-019-0461-3
Seow, K.M., Chang, Y.W., Chen, K.H., Juan, C.C., Huang, C.Y., Lin, L.T., Tsui, K.H., Chen, Y.J., Lee, W.L. and Wang, P.H. (2020) ‘Molecular mechanisms of laparoscopic ovarian drilling and its therapeutic effects in polycystic ovary syndrome’, International Journal of Molecular Sciences, 21(21). Available at: https://doi.org/10.3390/ijms21218147
Abu Hashim, H. (2014) ‘Predictors of success of laparoscopic ovarian drilling in women with polycystic ovary syndrome: an evidence-based approach’, Archives of Gynecology and Obstetrics, 291(1), pp. 11–18. Available at: https://doi.org/10.1007/s00404-014-3447-6
Zhang, J., Zhou, K., Luo, X., Yang, M., Shen, X. and Xu, L. (2020) ‘Variation of laparoscopic ovarian drilling for clomiphene citrate-resistant patients with polycystic ovary syndrome and infertility: a meta-analysis’, Journal of Minimally Invasive Gynecology, 27(5), pp. 1048–1058. Available at: https://doi.org/10.1016/j.jmig.2019.06.022
Baradwan, S., Abuzaid, M., Sabban, H., Alshahrani, M.S., Khadawardi, K., AlSghan, R., Alnoury, A., Bukhari, I.A., Alyousef, A., Belancic, A., Persad, E. and Abu-Zaid, A. (2023) ‘Transvaginal needle versus laparoscopic ovarian drilling in hormonal profile and pregnancy outcomes of polycystic ovary syndrome: a systematic review and meta-analysis’, Journal of Gynecology Obstetrics and Human Reproduction, 52(6), p. 102606. Available at: https://doi.org/10.1016/j.jogoh.2023.102606
Flyckt, R.L. and Goldberg, J.M. (2011) ‘Laparoscopic ovarian drilling for clomiphene-resistant polycystic ovary syndrome’, Seminars in Reproductive Medicine, 29(2), pp. 138–146. Available at: https://doi.org/10.1055/s-0031-1272476
Api, M. (2009) ‘Is ovarian reserve diminished after laparoscopic ovarian drilling?’, Gynecological Endocrinology, 25(3), pp. 159–165. Available at: https://doi.org/10.1080/09513590802585605
Medical Device Network (December 2025). May Health gains CE mark for infertility treatment. Retrieved from medicaldevice-network.com
MassDevice (December 2025). May Health earns CE mark for system for PCOS-related infertility. Retrieved from massdevice.com
Anna O'Sullivan (March 2026). May Health raises $11.7M to advance device treatment for PCOS-related infertility.
ClinicalTrials.gov. The REBALANCE Study (NCT06206746).
EXCELLENT article Fran. Everytime I hear this term I imagine an oil field. This name is just about as bad as "geriatric pregnancy" lol. I can only assume it was named by a dude?