
Lean PCOS #77
How is Lean PCOS different?

Good morning everyone,
How was your week? It’s almost the end of June, and I still wear jackets in London. Are you in a hotter country?
Today, we discuss Lean PCOS. I know I have spoken to quite a few of those who read this newsletter who fall into this category. Let’s deep-dive into it.
How prevalent is Lean PCOS?
The actual percentage varies greatly, but it is thought that between 20% and 50% of women with PCOS have the lean phenotype. That is quite a large number. The main difference that gives this categorisation is weight. The lean PCOS girlie doesn’t seem to have the problem of weight; however, they exhibit the same three characteristics of PCOS: irregular periods, high testosterone, and/or polycystic ovaries.
Unfortunately, Lean PCOS has significantly less research than the overweight phenotype. This seems to be the case because, in the US, the prevalence of overweight PCOS is far bigger than the lean phenotype.
What is the difference between those with weight issues and lean PCOS?
1. Weight
Both phenotypes are thought to have an issue with weight, but this is distributed differently. Lean PCOS presents a similar metabolic risk as they carry a similar amount of visceral adipose tissue (the fat around your organs). This is often the reason why both overweight and normal weight people can be diagnosed with the same ‘metabolic’ led diseases (such as type 2 diabetes, high cholesterol, etc). The fat that is detrimental to our health is the one that accumulates around our organs, not under our skin. The tricky part is that you can’t see that fat. Science believes that people carry different fat capacities. Some people can store fat under their skin to a higher capacity, whilst others have a lower capacity, meaning that fat goes around organs when overeating. This is why you can also have obese people who can be perfectly healthy. Overall, of course, BMI has been correlated with a number of diseases, but the debate is not as straightforward as it seems.
Genetic research has identified specific genes that influence fat distribution and storage. Variants in genes such as FTO, MC4R, and PPARG are associated with differences in body fat distribution and obesity risk.
A DEXA scan is the gold standard for measuring visceral fat levels. A study found a correlation between adiposity assessed by DEXA (total or central fat) and insulin sensitivity (QUICKI) in patients with PCOS.
2. Insulin Resistance
The research on this is a bit contradictory. Some studies report that both groups' insulin resistance rates are similar, irrespective of weight. Others, on the other hand, report that insulin resistance is worse and more prevalent in overweight PCOS patients. What is consistent is that obese individuals with PCOS suffer from more severe hormonal and metabolic issues compared to their lean counterparts.
An issue with β-cell function (the production of insulin) has been found in both overweight and lean PCOS women. This might be the reason.
It is essential to test for insulin resistance regardless of your phenotype.
3. Testosterone levels
When it comes to higher levels of testosterone, this is the same for both lean and overweight PCOS women. Some studies do report that a higher BMI can lead to higher levels of testosterone.
4. LH/FSH
This imbalance between the Luteinising hormone and follicle-stimulating hormone seems to be the same stimulating hormone is the same in both PCOS types. However, even for this, there is one study that shows this imbalance to be worse in obese PCOS patients.
Ok, so things seem to be the same. So why is the weight different?
While I wanted to find a straightforward answer to this difference, there isn’t. I think this is due to the lack of research.
I did find some differences in genetics. Two genes, LEP and ADIPQQ, are different:
LEP deals with the satiety hormone leptin, which tells your brain you are full. In obese women, LEP seems to be upregulated. Elevated leptin levels should theoretically reduce appetite, but in obese individuals, leptin resistance often develops. This resistance blunts the appetite-suppressing effects of leptin, leading to increased hunger and potential overeating. In Lean PCOS, these genes seem to work accordingly. It might mean that those with overweight PCOS, like me, have an increased appetite and, as a result, overeat.
ADIPQQ gene encodes adiponectin, a hormone produced by (fat cells). It enhances insulin sensitivity and has anti-inflammatory effects. Lower levels of adiponectin are observed in obese women with PCOS compared to lean PCOS girlies. Adiponectin increases energy expenditure, indirectly reducing appetite.
So, it might be down to appetite. Overweight or obese PCOS girlies might experience a greater appetitive. This is not fully established, so I would take it with a pinch of salt until further research develops.
We are officially starting a genetics-based PCOS Program on the 30th of September. If you are interested in learning what is driving your PCOS in genetics, you can sign up for the waiting list here.
Challenges
The challenge with lean PCOS women is that it usually takes much longer to get diagnosed as PCOS is not suspected immediately. We all know the confusion, worry and experience of getting diagnosed too late. It’s an incredibly hurtful experience not knowing what is wrong with you.
Management of lean PCOS
The management of lean PCOS is very similar to that of overweight/obese PCOS. Metformin was found to be more successful in restoring menstruation (55%) and ovulation (45%) in lean women with PCOS compared with their obese counterparts. This makes me think that insulin resistance is indeed present in both phenotypes.
Myo-inositol has also been found to be effective in Lean PCOS.
Of course, the weight loss recommendation doesn’t apply to lean PCOS individuals. However, I would still focus on reducing the fat around the organs and measure that as a measure of success (which I think should be the same for overweight people).
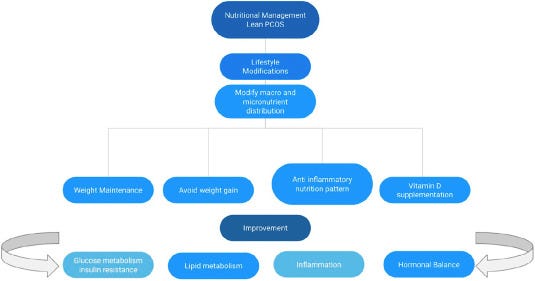
From a nutritional perspective, the advice is the same: focus on anti-inflammatory foods and a diet rich in nutrients.
Here is an extract from a study on the nutritional management for Lean PCOS.
Conclusion
As you can see, there isn’t much difference between the phenotypes, and they both need to be managed with the same lifestyle interventions. I hope more research on the Lean PCOS phenotype emerges so we find more clarity.
See you next Sunday,
Francesca
www.pcos-clinic.com
Genazzani, A. D., Santagni, S., Ricchieri, F., Campedelli, A., Rattighieri, E., Chierchia, E., Marini, G., Despini, G., Prati, A., & Simoncini, T. (2014). Myo‐inositol modulates insulin and luteinizing hormone secretion in normal weight patients with polycystic ovary syndrome. The Journal of Obstetrics and Gynaecology Research, 40(5), 1353–1360. https://doi.org/10.1111/jog.12319
Idicula-Thomas, S., Gawde, U., Bhaye, S., Pokar, K., & Bader, G. D. (2020). Meta-analysis of gene expression profiles of lean and obese PCOS to identify differentially regulated pathways and risk of comorbidities. Computational and Structural Biotechnology Journal, 18, 1735–1745. https://doi.org/10.1016/j.csbj.2020.06.023
Paul, T., Satyaraddi, A., Cherian, K., Kapoor, N., Kunjummen, A., Kamath, M., & Thomas, N. (2019). Body composition, metabolic characteristics, and insulin resistance in obese and nonobese women with polycystic ovary syndrome. Journal of Human Reproductive Sciences, 12(2), 78. https://doi.org/10.4103/jhrs.jhrs_2_19
Singh, T., & Majumdar, A. (2009). Comparison of clinical features and health manifestations in lean vs. obese Indian women with polycystic ovarian syndrome. Journal of Human Reproductive Sciences, 2(1), 12. https://doi.org/10.4103/0974-1208.51336
Toosy, S., Sodi, R., & Pappachan, J. M. (2018). Lean polycystic ovary syndrome (PCOS): an evidence-based practical approach. Journal of Diabetes and Metabolic Disorders, 17(2), 277–285. https://doi.org/10.1007/s40200-018-0371-5
Disclaimer: We are all unique in our ways, so this information is for educational purposes only. In my communications, I summarise research data and bring my experience. This shouldn’t be viewed as medical advice at any point. Please further consult your healthcare provider about your health needs.